и„‘йғЁж”ҫз–—пјҢдёҠеҚҲжҜ”дёӢеҚҲж•Ҹж„ҹи®ёеӨҡпјҒ; ]4 U! r3 J' x
1 R. r4 z! t! s K5 T
1 _6 n+ t1 x# ?0 }, TCancer 2011 Jan 15;117(2):414-20. doi: 10.1002/cncr.25423. Epub 2010 Sep 9.
" x+ j- ~$ c: t. N; g$ j4 \Gamma knife radiosurgery for brain metastasis of nonsmall cell lung cancer: is there a difference in outcome between morning and afternoon treatment?4 e( o" N( h1 V: x' J. K
Rahn DA 3rd, Ray DK, Schlesinger DJ, Steiner L, Sheehan JP, O'Quigley JM, Rich T.. }. Y$ F/ a7 f8 B, G. G& ]
SourceDepartment of Radiation Oncology, University of Virginia Health Sciences Center, Charlottesville, Virginia 22908, USA.& k0 o/ F- R* J1 K8 \
1 n' J; K9 W2 v. u$ I4 C& u2 S
Abstract
. I9 F* k$ s, e2 VBACKGROUND: Circadian cell-cycle progression causes fluctuating radiosensitivity in many tissues, which could affect clinical outcomes. The purpose of this study was to determine whether outcomes of single-session gamma knife radiosurgery (GKRS) for metastatic nonsmall cell lung cancer (NSCLC) differ based on treatment time.8 O7 v( P. |& w& y. H. C0 ]* m6 d
j$ s+ G6 ^( r3 y6 J/ mMETHODS: Fifty-eight patients received GKRS between 10:00 am and 12:30 pm and 39 patients received GKRS between 12:30 pm and 3:00 pm. The mean peripheral dose was 18.6 Gy. The mean tumor size was 7.3 cm³. Magnetic resonance imaging was used to score local control at 3 months. Cause of death (COD) was categorized as central nervous system (CNS)-related or systemic.
; C3 O" f; [2 M% j0 { u
" Q/ E7 t: J; }! A7 z# d3 a% Y0 g% KRESULTS: Demographic and disease characteristics of the 2 groups were similar. Local control at 3 months was achieved in 97% (35/36) of patients who underwent GKRS early in the day versus 67% (8/12) of patients who underwent GKRS later in the day (chi-square, P = .014). Early GKRS was associated with better survival (median 9.5 months) than late GKRS (median 5 months) (Kaplan-Meier log-rank test, P = .025). Factors contributing to better survival in a Cox regression model included early treatment time (P = .004) and recursive partition analysis class (P < .001). Cause of death in the early treatment group was CNS-related in 6% (3/47) of patients versus 24% (8/34) of patients in the late treatment group (chi-square test, P = .026).2 k0 f( O2 t1 q+ e( X
5 E8 F; v/ d! \CONCLUSIONS: GKRS for metastatic NSCLC had better local control, better survival, and a lower rate of CNS-related cause of death when given earlier in the day versus later in the day. These retrospective data should encourage future study in brain radiosurgery and non-CNS stereotactic body radiotherapy series.
8 r/ c) s3 J( e& S8 {( {+ l V2 n
|


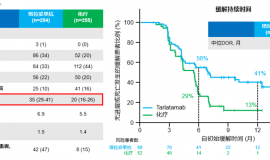
 ж №жІ»жҖ§ж”ҫз–—з»“жқҹеҗҺпјҢе…Қз–«з»ҙжҢҒдёӨе№ҙиғҪдёҚ
家зҲ¶2022е№ҙ12жңҲд»ҪзЎ®иҜҠеҸіиӮәдёҠеҸ¶иӮәйіһзҷҢ3AжңҹпјҢзәөиҶҲж·Ӣе·ҙз»“иҪ¬з§»пјҢдёҖзӣҙеңЁеӨҚиӮҝжІ»з–—пјҢе…Ҳж–°иҫ…еҠ©
ж №жІ»жҖ§ж”ҫз–—з»“жқҹеҗҺпјҢе…Қз–«з»ҙжҢҒдёӨе№ҙиғҪдёҚ
家зҲ¶2022е№ҙ12жңҲд»ҪзЎ®иҜҠеҸіиӮәдёҠеҸ¶иӮәйіһзҷҢ3AжңҹпјҢзәөиҶҲж·Ӣе·ҙз»“иҪ¬з§»пјҢдёҖзӣҙеңЁеӨҚиӮҝжІ»з–—пјҢе…Ҳж–°иҫ…еҠ©
 жҜҚдәІжҷҡжңҹиӮәзҷҢи·Ёи¶Ҡ11е№ҙдәҶпјҒжҲ‘们зҡ„5зӮ№
и®Іиҝ°иҖ…пјҡе°ҸзҷҪе…”ж•ҙзҗҶиҖ…пјҡpear
2014е№ҙжҜҚдәІзЎ®иҜҠжҷҡжңҹиӮәи…әзҷҢпјҢдёҖи·Ҝж‘ёзҙўжҠ—зҷҢеүҚиЎҢпјҢе№ёеҫ—з—…еҸӢ
жҜҚдәІжҷҡжңҹиӮәзҷҢи·Ёи¶Ҡ11е№ҙдәҶпјҒжҲ‘们зҡ„5зӮ№
и®Іиҝ°иҖ…пјҡе°ҸзҷҪе…”ж•ҙзҗҶиҖ…пјҡpear
2014е№ҙжҜҚдәІзЎ®иҜҠжҷҡжңҹиӮәи…әзҷҢпјҢдёҖи·Ҝж‘ёзҙўжҠ—зҷҢеүҚиЎҢпјҢе№ёеҫ—з—…еҸӢ
 жӯ»дәЎйЈҺйҷ©йҷҚдҪҺ40%пјҒе°Ҹз»ҶиғһиӮәзҷҢеӨҚеҸ‘жӮЈ
дҪңиҖ…пјҡV
е°Ҹз»ҶиғһиӮәзҷҢпјҲSCLCпјүжҳҜдёҖз§Қе…·жңүй«ҳеәҰдҫөиўӯжҖ§е’Ңз ҙеқҸжҖ§зҡ„жҒ¶жҖ§иӮҝзҳӨпјҢзәҰеҚ е…ЁзҗғжүҖжңүиӮә
жӯ»дәЎйЈҺйҷ©йҷҚдҪҺ40%пјҒе°Ҹз»ҶиғһиӮәзҷҢеӨҚеҸ‘жӮЈ
дҪңиҖ…пјҡV
е°Ҹз»ҶиғһиӮәзҷҢпјҲSCLCпјүжҳҜдёҖз§Қе…·жңүй«ҳеәҰдҫөиўӯжҖ§е’Ңз ҙеқҸжҖ§зҡ„жҒ¶жҖ§иӮҝзҳӨпјҢзәҰеҚ е…ЁзҗғжүҖжңүиӮә
 йіһзҷҢ3жңҹжңҜеҗҺ16дёӘжңҲеӨҡдёӘиӮҝж ҮеҚҮй«ҳ
7.9дҪҸйҷўеӨҚжҹҘдәҶctе’ҢиЎҖжҢҮж ҮпјҢеүҚжңҹиҖҒзҲ¶дәІиў«иҶқе…іиҠӮз–јз—ӣжҠҳзЈЁзҡ„дёҚиҪ»пјҢmrжЈҖжөӢиҶқзӣ–йғЁеҲҶж— еҸҜз–‘
йіһзҷҢ3жңҹжңҜеҗҺ16дёӘжңҲеӨҡдёӘиӮҝж ҮеҚҮй«ҳ
7.9дҪҸйҷўеӨҚжҹҘдәҶctе’ҢиЎҖжҢҮж ҮпјҢеүҚжңҹиҖҒзҲ¶дәІиў«иҶқе…іиҠӮз–јз—ӣжҠҳзЈЁзҡ„дёҚиҪ»пјҢmrжЈҖжөӢиҶқзӣ–йғЁеҲҶж— еҸҜз–‘
 жһ—ж №ж•ҷжҺҲпјҡиӮәзҷҢи„‘иҶңиҪ¬з§»иҜҠж–ӯеҸҠз”ЁиҚҜзӯ–
ж•ҙзҗҶиҖ…пјҡйӣЁиҝҮеӨ©жҷҙе®Ўж ёдәәпјҡй№°зүҲзҷҢз»Ҷиғһеҗ‘дёӯжһўзҘһз»Ҹзі»з»ҹзҡ„иҪ¬з§»пјҢе°Өе…¶жҳҜи„‘иҶңиҪ¬з§»пјҢжҳҜеҪұе“Қжҷҡ
жһ—ж №ж•ҷжҺҲпјҡиӮәзҷҢи„‘иҶңиҪ¬з§»иҜҠж–ӯеҸҠз”ЁиҚҜзӯ–
ж•ҙзҗҶиҖ…пјҡйӣЁиҝҮеӨ©жҷҙе®Ўж ёдәәпјҡй№°зүҲзҷҢз»Ҷиғһеҗ‘дёӯжһўзҘһз»Ҹзі»з»ҹзҡ„иҪ¬з§»пјҢе°Өе…¶жҳҜи„‘иҶңиҪ¬з§»пјҢжҳҜеҪұе“Қжҷҡ






 жҳҫиә«еҚЎ
жҳҫиә«еҚЎ